Platlet Activating Factor and Intrauterine Inseminations by William E. Roudebush, PhD

William E. Roudebush, Ph.D., HCLD
Clinical Associate Professor, Physiology
University of South Carolina
T 864.455.9842
F 864.455.5267
Dr. Roudebush’s work involving PAF and fertility has received many awards and honors. He has published over 160 articles, book chapters and abstracts relating to research in the field of infertility.
In many centers drug induced ovulation induction (OI) followed by intrauterine insemination (IUI) have become standard therapy for non-tubal factor related infertility. As the initial treatment for infertile couples, IUI is commonly used and is a cost effective procedure. The success of IUI is dependent on the ovulation induction regimen as well as seminal parameters. Commonly, because of lower patient costs, complexity and risks of high order multiple pregnancy, clomiphene citrate (CC) is initially used. At Reproductive Biology Associates (RBA), Atlanta, GA the typical treatment regimen involves three CC/IUI cycles followed by GT/IUI for up to three cycles. Failed IUI therapy subsequently results in consideration of in vitro fertilization therapy.
Male fertility requires production of an adequate number of normal sperm with sufficient motility for fertilization. Poor production of quality sperm may lead to subfertility or infertility. A number of endogenous biochemical factors have been attributed to regulate the fertility potential of spermatozoa, for example platelet-activating factor. Platelet-activating factor (PAF) is present in human spermatozoa, and its content has a significant and positive relationship with motility and pregnancy rate. In a recently published paper (Fertility & Sterility 2004;82:52-56), we reported on the benefit of washing sperm with PAF for intrauterine insemination.
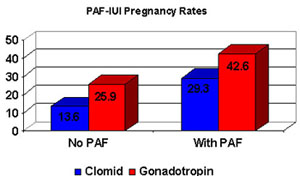
Since February 10, 2003 RBA has been routinely adding PAF to the IUI sperm wash protocol. The average pregnancy rate for PAF-IUI cycles is >40% (see graph below), nearly twice the rate of non-PAF treated IUI cycles (~29%). Additionally, we are finding a tremendous improvement in first-cycle IUI pregnancy rates. Patients are finding less time (a 1 in 3 chance with PAF compared to a less than 1 in 5 chance without PAF) required to become pregnant with PAF-IUI, thereby resulting in reduced cost for infertility treatment.
PAF is a potent phospholipid that is naturally found in sperm and whose content has a positive correlation with pregnancy outcome. From our studies on PAF, we have found that morphologically abnormal sperm do not respond to PAF as do normal-motile sperm, with improvements in overall sperm motility (numbers and grade). We believe PAF has a sperm-selective capacity that results in the improved pregnancy outcomes. PAF is a safe and efficacious treatment for patients undergoing IUI therapy for infertility.
William E. Roudebush, Ph.D., HCLD
Clinical Associate Professor, Physiology
T 864.455.9842
F 864.455.5267
Dr. Roudebush’s work involving PAF and fertility has received many awards and honors. He has published over 160 articles, book chapters and abstracts relating to research in the field of infertility.